Anterior Communicating Artery Aneurysms
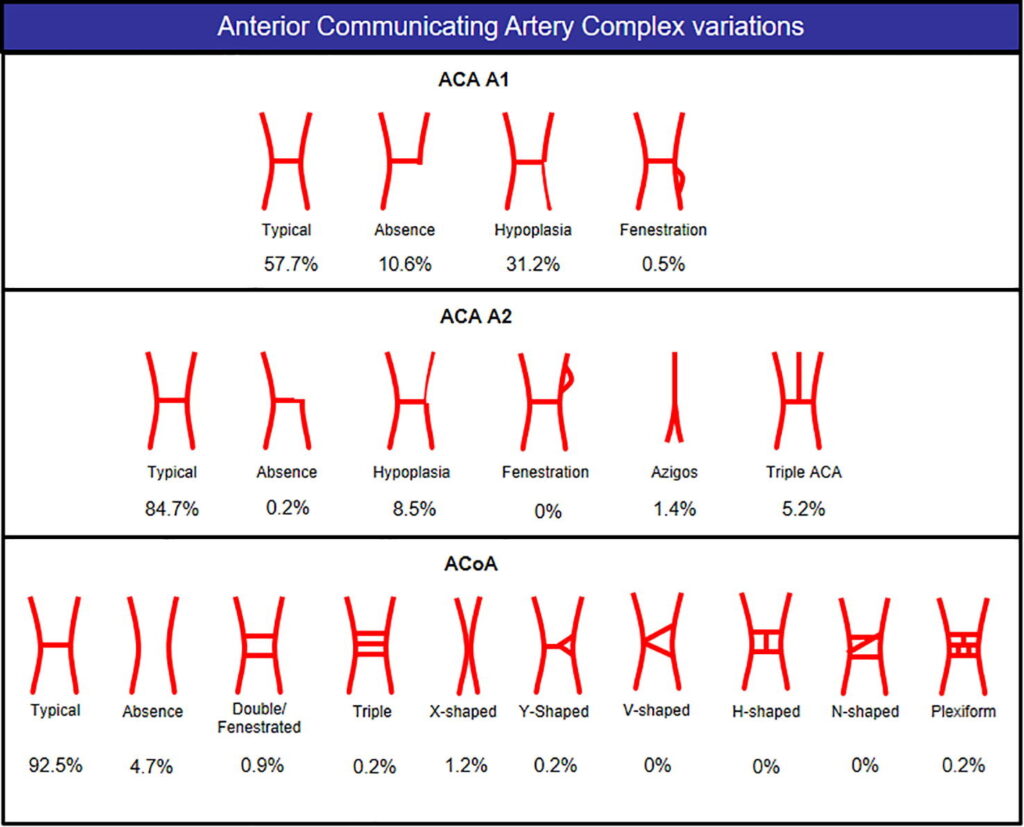
The anterior communicating artery is a complex and highly variable structure that may create challenges during endovascular treatment. Fenestrations and early bifurcations are common, as are variations in the relative size of the A1 segments. Thus, thorough planning is essential for the safe treatment of anterior communicating artery aneurysms. We recommend 3D angiography as an essential tool to accurately map the inflowing and outflowing vessels and to obtain appropriate working projections.
CASE
History: 70s year-old woman with history of mild dementia, hypertension, dyslipidemia, heart failure with preserved ejection fraction, and a history of ischemic stroke with residual right sided weakness. She was incidentally found to have an anterior communicating artery and patient and family wished to proceed with consideration for treatment.
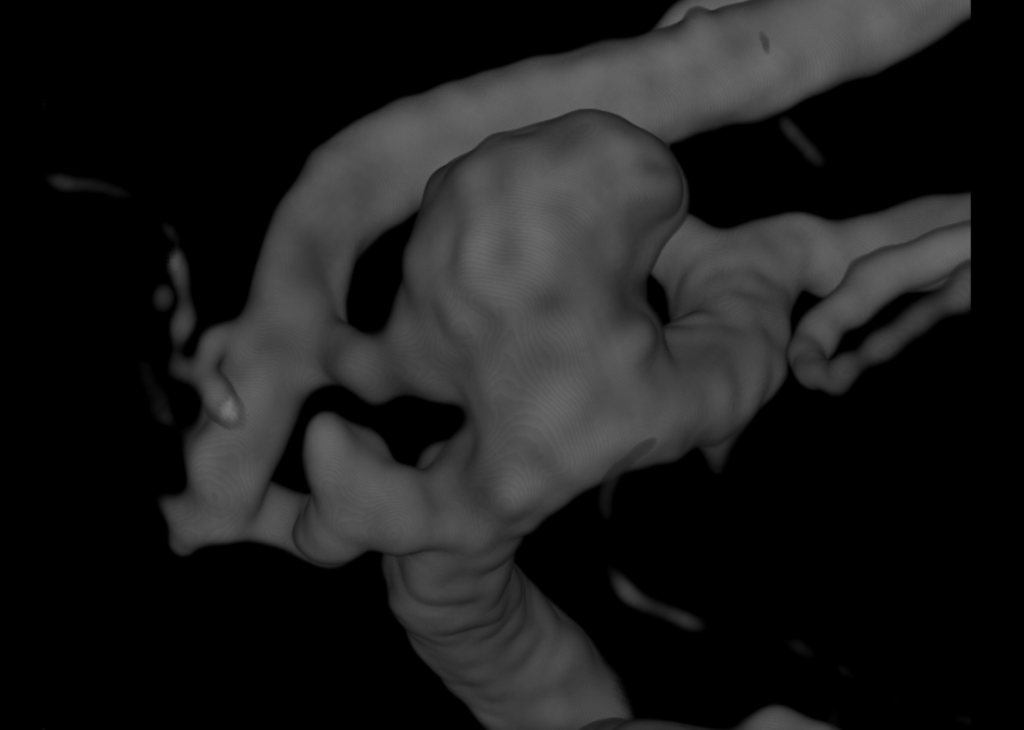
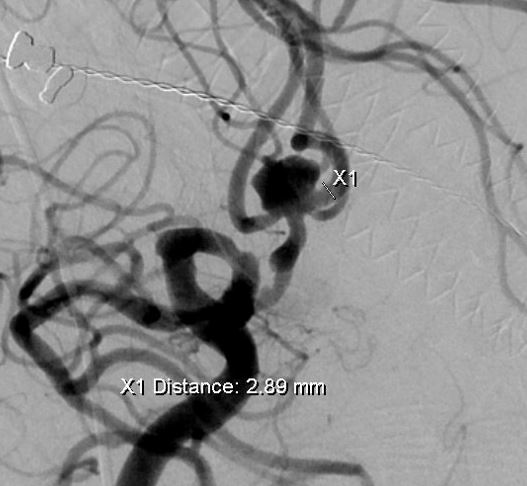
The patient arrived for her cerebral angiogram and the following anterior communicating artery aneurysm was visualized using 3D rotation angiography.
As you can see, the aneurysm is wide-necked, irregularly shaped, with multiple branches arising from the neck of the aneurysm.
There is no left A1:

In this case, an 8 French Shuttle sheath was used for support and connected to a Trident RHV. An angled glide catheter and a 0.038 angled Glidewire were used to select the right common
carotid artery and the 8 French shuttle sheath was advanced into the right common carotid artery.
A Phenom plus microcatheter was used as intermediate catheter for extra support. Then, an Excelsior SL-10 was advanced into the left A2 across the anterior communicating artery with a Synchro 14 soft microwire. After that, an Echelon 10 microcatheter was advanced into the body of the aneurysm through the other port of the 8 French shuttle sheath with a Synchro 14 soft microwire.
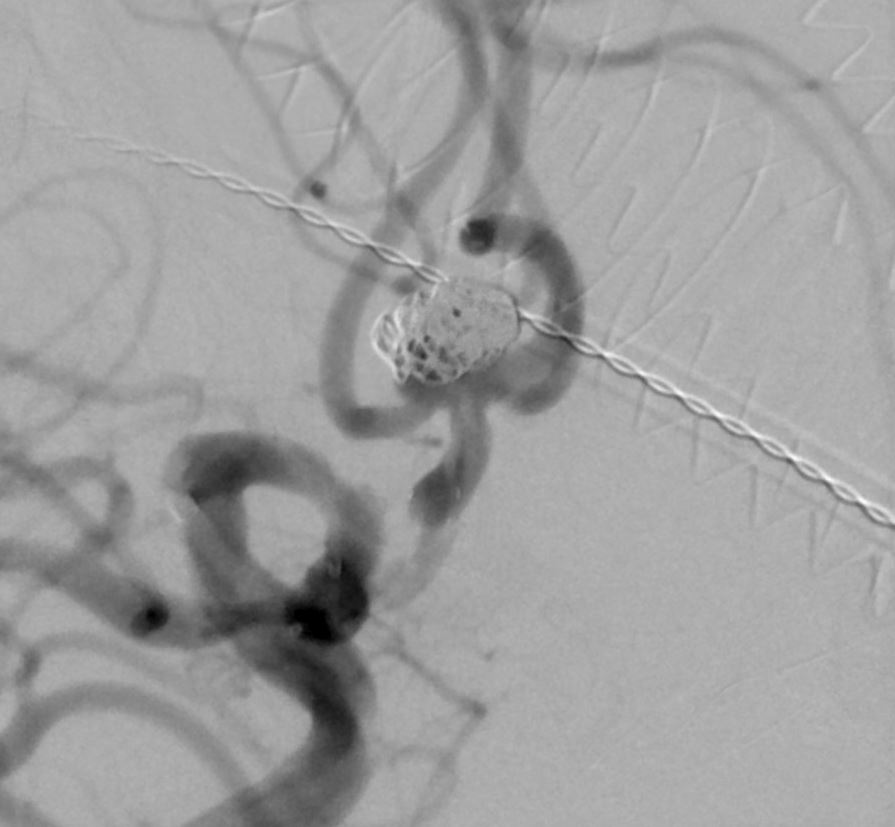
Then, a Stryker 3mm x 24mm Neuroform ATLAS stent was advanced into the SL-10 and deployed from the left A2 to the right A1 artery. The SL-10 microcatheter was then removed.
The phenom plus intermediate catheter was kept in place to perform control
angiograms through the right internal carotid artery. The following coil was then deployed:
- Target 3D 7mmx15cm
There was difficulty in keeping the coil mass away from the right pericallosal branch
on the right side; and thus a second microcatheter (Headway Duo 156) was inserted into the Phenom plus and then placed through the stent into the aneurysm. The the following coils were then deployed:
- Target 360 Soft 5mm x 10cm
- Target 360 Soft 3mm x 10cm
- Target 360 Soft 3mm x 8cm
The initial Target 3-D coil was then detached from the first microcatheter.
A final Target 360 3mm x 6cm was then deployed through the first microcatheter. Given the patient’s advanced age and comorbidities, the decision was made to stop the procedure at this time with adequate occlusion of the aneurysm.