The trigeminal artery is present in all people and traverses with the trigeminal nerve. In early development, the trigeminal artery serves as the main blood supply for the hindbrain. It typically involutes later in development. In rare cases, the trigeminal artery persists and provides a formidable arterial connection between the internal carotid artery and the posterior circulation.
Persistent Trigeminal Arteries have a classification scheme:
- Saltzman type I: Supplies the distal vertebrobasilar arteries. The posterior communicating artery is absent and the caudal basilar is absent or hypoplastic with hypoplastic distal vertebral arteries.
- Saltzman type II: Supplies the superior cerebellar arteries with the posterior cerebral arteries supplied by the posterior communicating artery
- Saltzman type III: Does not join the basilar artery, instead directly terminating as the
- type IIIa: superior cerebellar artery
- type IIIb: anterior inferior cerebellar artery
- type IIIc: posterior inferior cerebellar artery
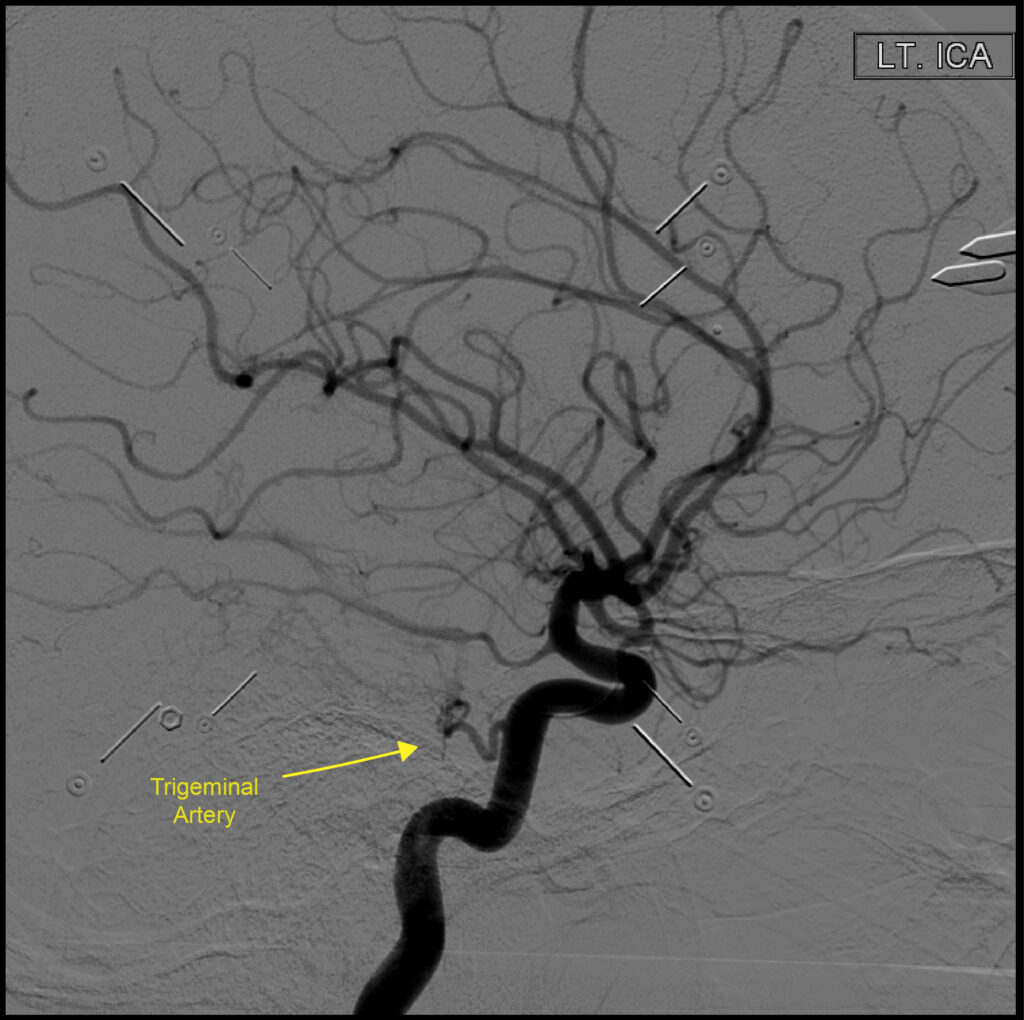
Here is an example of an example of a Saltzman type II Trigeminal Artery:
Here is a separate Persistent Trigeminal Artery Type I example: CT angiogram of the head.
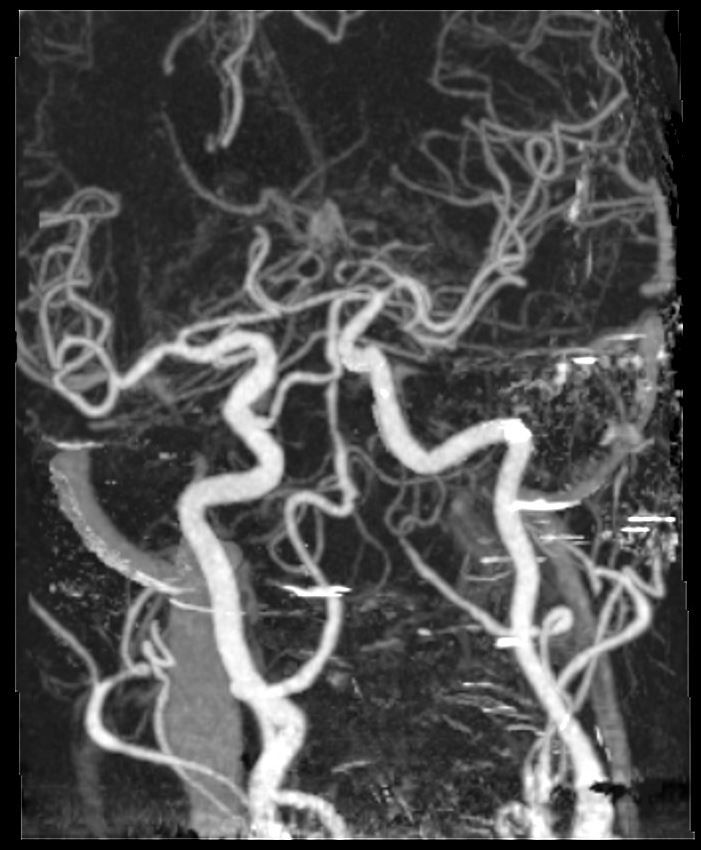
In this case, the persistent trigeminal artery arises from the right internal carotid artery and feeds into the basilar artery between the AICA and the superior cerebellar artery. There is an accompanying stenosis (or rather congenital narrowing) of the basilar artery just proximal to its entry point.
Clinically, it is important to be aware of the persistent trigeminal artery for several reasons. E.g. for a WADA test, of course, you would not want to inject Amytal into the posterior circulation and cause a coma. An internal carotid artery plaque could cause downstream stroke in the posterior circulation in the presence of a persistent trigeminal artery.