CASE
A man in his late 70s presented with acute onset right sided weakness and aphasia. Imaging demonstrated occlusion of the Left ICA up to the left M1 artery.
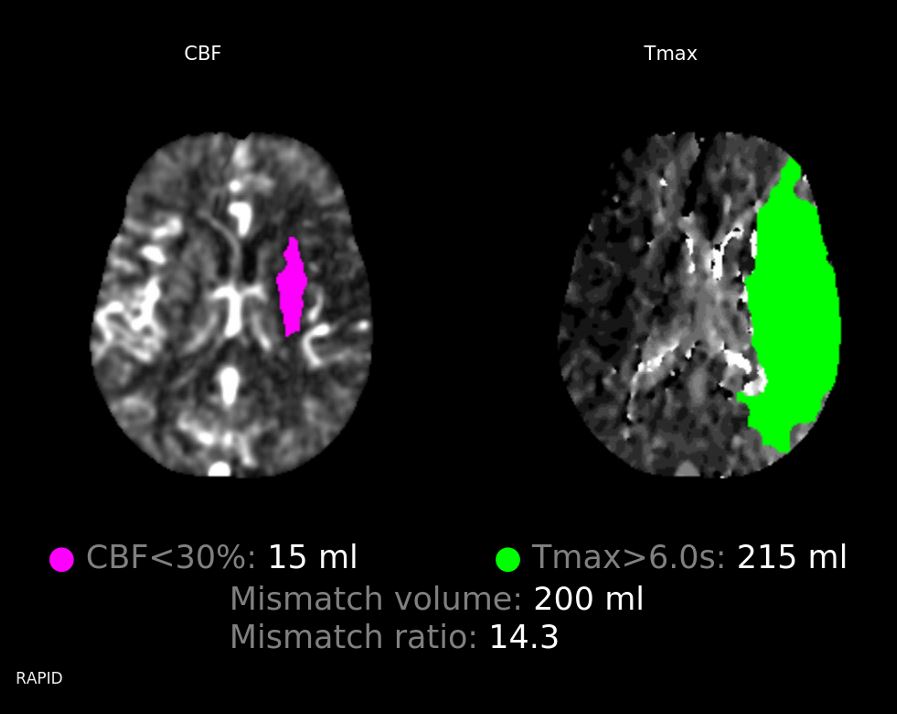
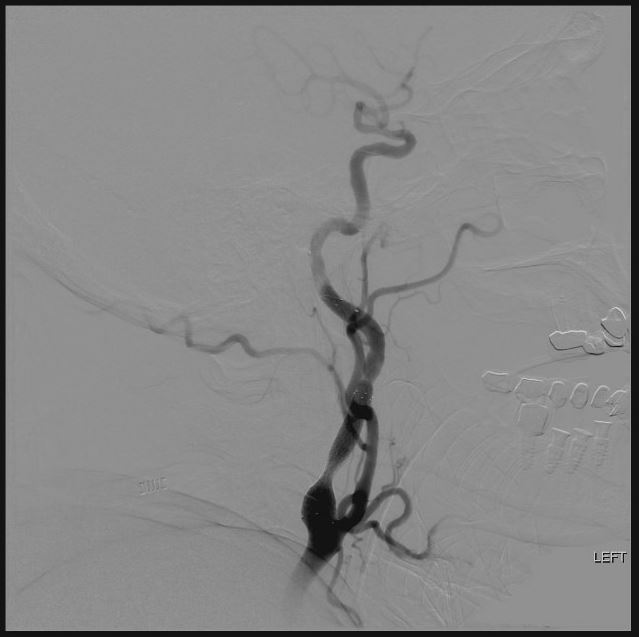
Patient was taken for acute thrombectomy attempt and was found to have a left ICA occlusion with taper just past the carotid bulb. It was unclear if this occlusion extended up to the carotid terminus and into the M1 or rather (more likely) that the left ICA demonstrated acute on chronic occlusion with distal emboli to the left M1.

There was an initial aspiration attempt made on the left ICA occlusion with a Zoom 71 catheter, which only partially open up the left ICA occlusion.
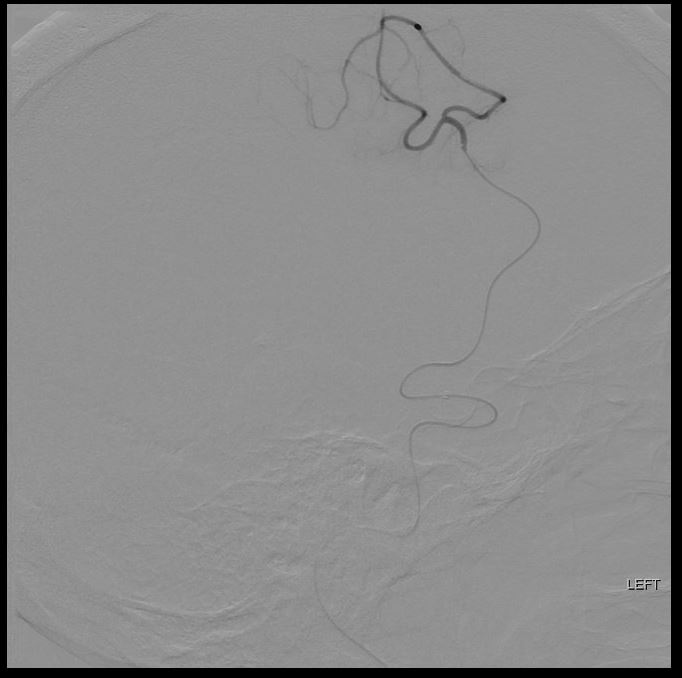
Following this first attempt, the microsystem (Trevo Trak 21 and Synchro 14 standard microwire) was advanced beyond the occlusion to attempt a combined thrombectomy attempt with aspiration and stent retriever (Zoom 71 + Solitaire 4 x 40) (below).
Zoom 71 and Solitaire 4 x 40 combined approach

Partial recanalization of the left M1 with persistent occlusion of the posterior division M2.
A Zoom 55 aspiration catheter was prepared and advanced into the distal left M2 with the help of the Trevo Trak 21 and the Synchro 14 standard microwire. Aspiration was completed into the Emboguard Balloon guide catheter, completing a third pass. More red clot was observed in the aspirate.
Unfortunately, post thrombectomy angiogram demonstrated new occlusion of the left ACA territory (A2/A3) and a 4th pass was conducted to remove this clot with the Zoom 55 aspiration catheter and the Solitaire 4mmx40mm stent retriever. The aspirate again demonstrated more red clot.

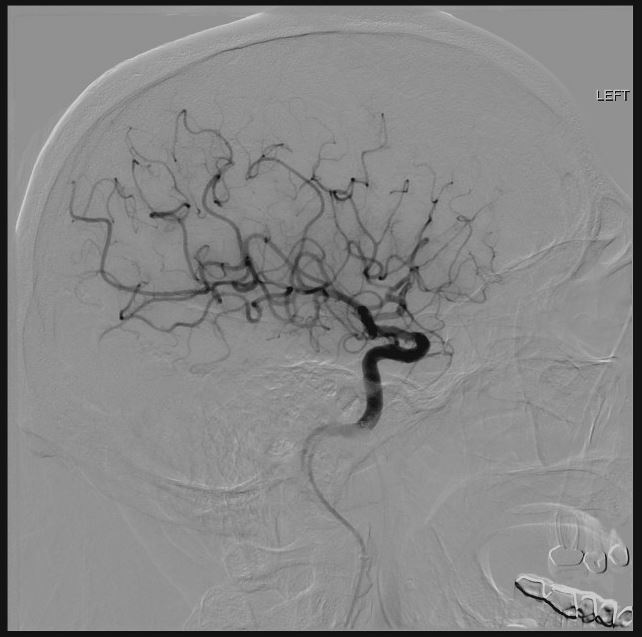
With adequate recanalization of the intracranial circulation, attention was then paid to the proximal left ICA.
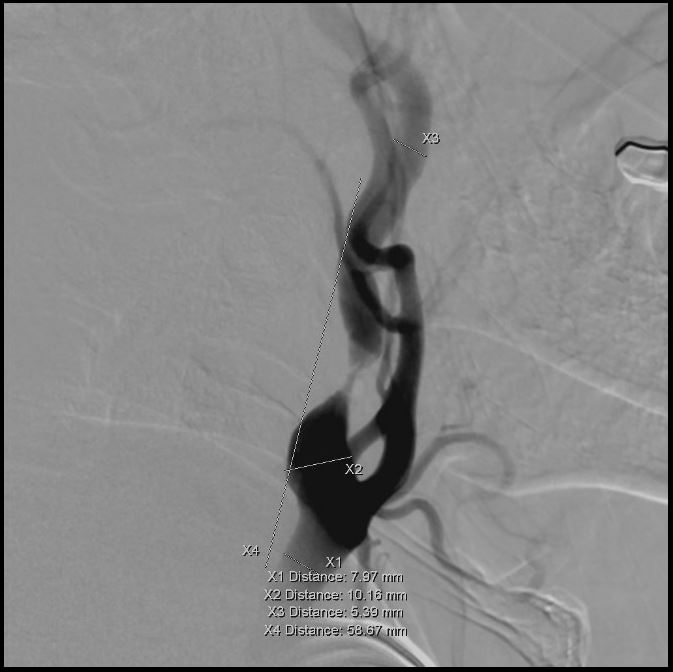
The left ICA intermittently occluded and thus the decision was made to undergo angioplasty and stenting. Measurements observed above.
Angiogram of the left internal carotid artery prior to angioplasty and stenting with the 7mm Spider FX distal embolic protection device in place.
Over the distal embolic protection device, a TREK 4mm x 20mm balloon was advanced over the wire the distal embolic protection device to the cervical left internal carotid artery lesion. It was inflated below nominal to approximately 3.2 mm (below).

The patient was bolus Cangrelor and started on a Neuro dosing protocol (1/2 the cardiac dose). The balloon was then deflated and removed from the body. A post angioplasty angiogram demonstrated adequate widening of the lesion. There was note of filling defect within the distal embolic protection device.
A 3T MRI compatible ev3 PROTEGE RX 10->7 x 40 carotid stent was then deployed over the wire. Stenting was conducted with the balloon guide inflated for proximal projection.
Patient was neurologically improved following the procedure with improved speech and right sided strength. The post-op CT demonstrated anterior falcine constrast versus subarachnoid hemorrhage. A follow-up CT Head demonstrated slight worsening of the subarachnoid hemorrhage and the Cangrelor was decreased to a quarter dose.
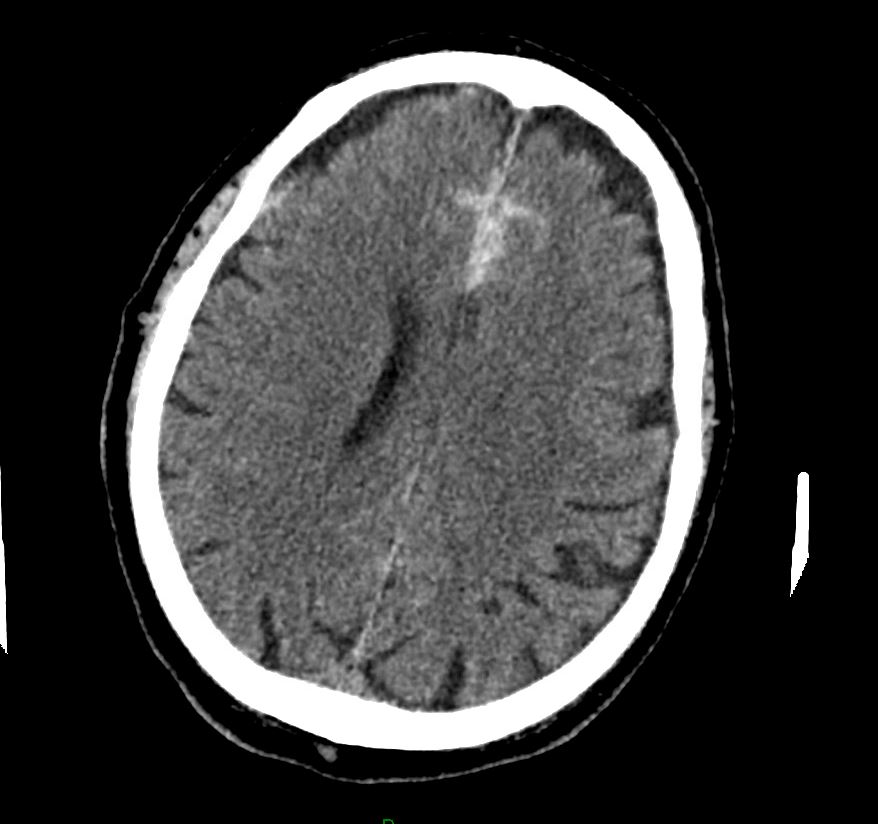
Follow-up CT head scans were stable. The patient demonstrated infarct in the left basal ganglia and frontal corona radiata region but his strength and aphasia improved. He was later transferred out of the hospital without further neurological decline after being transitioned to Aspirin + Ticagrelor.